The tricky part about "reading" your patient's nervous system and their sensory needs is that this process keeps you on your toes! The difficulty with sensory diets or "programs' is that they don't always allow you to "read" the nervous system of the child in the moment. Questions like "what is the child's current state?" before you begin a sensory intervention is key in deciding which types of activities might be helpful in moving the child's state towards homeostasis. Too often when following prescribed activities, flexibility is limited in meeting the childs CHANGING needs.
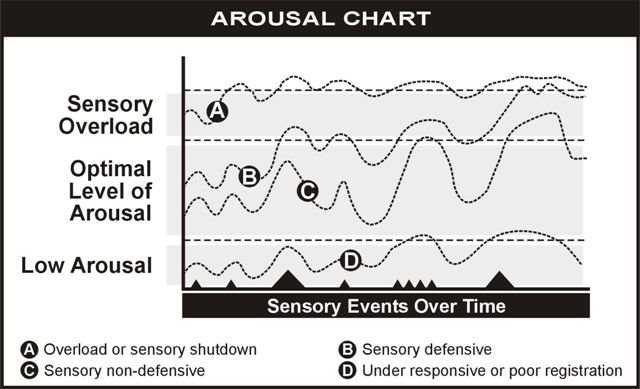
Many children with autism experience fluctuations in their sensory processing. This means that their sensory needs are in flux. The effective sensory strategy on one day, can bomb completely on another day. "Being present" to the child's current state helps the therapist decide in that moment where the child may be in their overall state of arousal. Are they hypo? hyper? or over-stimulated? Remember that when children are over-stimulated, they often pass through a hyper arousal state (giggling, laughing, flushing, etc) on their way to an organized state. Perhaps calming activity needs to be continued for a longer period of time as the child passes through the hyper-aroused state transiently.
Children with autism may have a wide variety of sensory processing issues. They may have difficulty with the initial "registration" of a sensation; where the brain is unable to "notice" the feeling of that sensation. At times there is a delay in processing time of a sensation, where there is a 'kick back" or a long duration for the brain to notice the sensation. Often we continue providing a sensory experience beyond the duration necessary as we perceiving the child's sensory threshold to be high; whereas in reality, the threshold may be low, and have a long latency in time for detection. The three variables we can play with when providing an experience are frequency, intensity and duration of a sensory stimulus. How often do we provide an experience? For how long? and to what intensity? Sensory intervention is not as simple as providing a regime of sensory feedback!
Sometimes children with sensory processing challenges become excited when they are actually connected to themselves! The excitement or increased arousal that we observe may be about feeling present and in their body. This is an increase in emotional arousal resulting from experience rather than an arousal created by too much sensory feedback. Discerning this situation requires an especially fine magnifying glass. Children who seek to repeat and repeat and repeat an activity often are emotionally charged by the successful processing of the experience. "I like this feeling!"
One other situation that deserves consideration is that sometimes many different sensory interventions need to be combined together in order to "ground" the nervous system. For example, many children need to combine listening intervention with movement, deep pressure touch, heavy work and purposeful task in order for the sensation to "have meaning". Raw sensory data can "bounce around in the nervous system" without grounding or organizing the child's overall behavior. One stimulus at a time may not be sufficient to be organizing.
As ususal, one question leads to another like a road map or pieces of a puzzle. The nervous system of children with sensory processing challenges creates a wonderful opportunity to become a detective!